
Exercise During Pregnancy: Give It Your All or Avoid It?
Reading Time: 4 minutes 49 seconds
BY: ISSA
DATE: 2019-04-03
Most fitness enthusiasts and almost all trainers are familiar with the "all or nothing" fallacy when it comes to exercise. It's the mistaken idea that if you can't do things to the max, you shouldn't do them at all.
Either you should do almost no exercise for the months during and after pregnancy, or you should pretty much ignore your pregnancy and carry on as normal.
Both are far from the best approach. Here's why.
Too little exercise and too much exercise during and after pregnancy are both bad ideas. The truth and best practices exist somewhere in the middle.
It's important for women to continue to exercise during pregnancy, but how hard you push your client is completely dependent on your client.
Where Exactly Do You Draw the Line?
During pregnancy, it's common for the hip flexors to take over for spinal stability. Adductors, abductors, and glutes become tight, which can cause biomechanical changes in the gait pattern during pregnancy[1] thus causing limitations for high impact training. When women continue to train, these muscle groups are impacted; they become tighter and less functional.
This makes it harder for the body to remain mobile and stable during pregnancy and birth. Sadly, mobility and stability are often not included in prenatal fitness training. This may leave women vulnerable to pelvic floor pain/lower back pain and discomfort.
Training during pregnancy can increase the risks of pelvic floor related symptoms, which can affect your client's postpartum recovery. Unfortunately, some of these women continue to train with pelvic floor dysfunctions like stress urinary incontinence (unintentional leaking), pelvic organ prolapse, and pelvic floor/hip pain because they're dismissed as a "normal" part of pregnancy and motherhood.
And a strong majority of these women will give up on their training in hope to avoid symptoms all together.
Here's What to Consider
The Pelvic Floor
The pelvic floor is like a woven basket that provides structural support, organ support, helps to maintain urinary and fecal incontinence, aids in sexual function, and stabilizes connecting joints. It is a dynamic muscle that needs to move as the body moves. With the structural and hormonal changes of pregnancy, along with high impact exercise during pregnancy, the pelvic floor can become overactive, weak, or both.
Diastasis Recti (a.k.a. Abdominal Separation or "Mummy Tummy")
Classified as the unnatural separation of the left and right rectus muscles 2cm or more. During pregnancy, the Linea Alba which is the connective tissue that runs down the midline of the abdomen, will begin to stretch away from the left and right rectus muscles.
Diastasis recti is a natural part of the pregnancy process. However, heavy lifts, toes to bar, crunching, and overhead lifts, which are all common in high impact fitness programs, can exacerbate this situation when training during pregnancy. Additionally, consider the effects of the hormone Relaxin, which makes joints, ligaments, and muscles lax in preparation for labor and birth. The pelvic floor and deep core system (made up of the diaphragm, pelvic floor, multifidus, and the transverse abdominis) may be weakened, making the pelvic floor vulnerable to dysfunctions.
For more on this issue, read "Battling The Postpartum Pooch...Why Sit Ups Are Bad" on the ISSA blog.
What Should You Do? And When?
Your clients can continue high impact fitness programs during pregnancy, but it's best to down-train as pregnancy progresses beginning in the second trimester.
Place special emphasis on breathing. Diaphragmatic breathing encourages recruitment of the deep core (diaphragm, pelvic floor, multifidus, and transversus abdominis).
As structural changes occur beginning in the second trimester, it's common for the pelvis to tilt or tuck under, inhibiting mobility. This also places stress on the deep core system because the diaphragm and pelvic floor are no longer in a stacked position.
When this happens, the transverse abdominus and multifidus are also unable to function optimally. This is where it's common to experience low back/hip pain[2]. This is another functional issue common for women during and after pregnancy.
It's best to begin addressing alignment starting in the first trimester.
You can help your client optimize alignment through these structural changes and reduce some common aches and pains, typical in pregnancy and postpartum. Plus, this helps optimize core function and minimizes diastasis recti.
Train Breathing Patterns and Introduce the Kegel
Disclaimer: Your client's doctor may not recommend Kegels if their pelvic floor is overly tight. That's okay. They can learn to relax their pelvic floor to create movement to be able to perform a Kegel.
A Kegel is a muscle contraction in the pelvic floor. A woman can hold it isometrically and let it relax. Your client will need her pelvic floor to do both efficiently during her training sessions with and without pelvic health symptoms.
There is some confusion surrounding how to properly Kegel. Women are taught to contract their pelvic floor without knowing how to relax. This is where the pelvic floor becomes overactive.
Additionally, women will bear down (pushing downward on the pelvic floor, instead of lifting it up and in), thinking they are doing a Kegel.
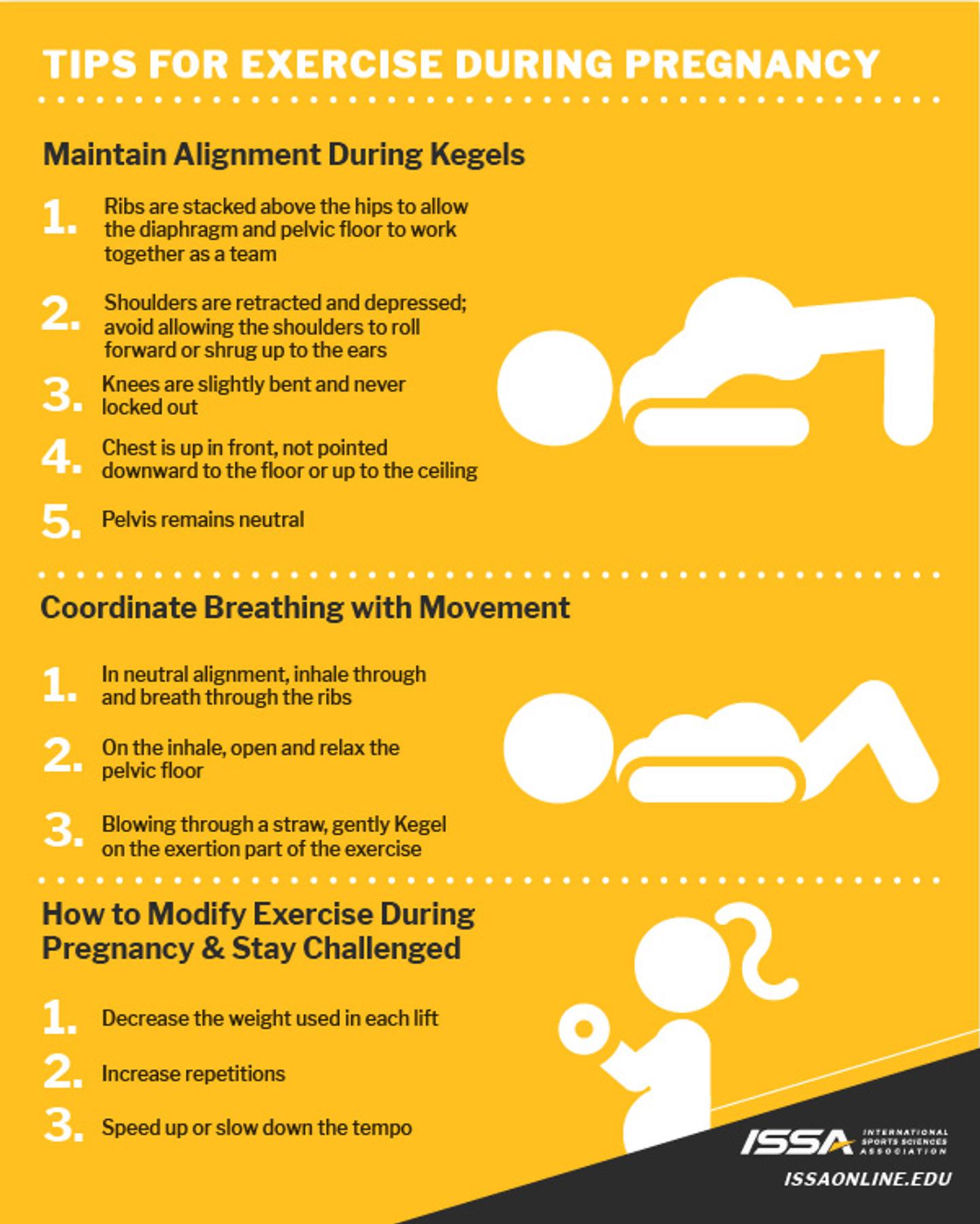
How to Coach a Kegel
All you're really having your client do, is a diaphragmatic breath with a Kegel on the exhale. This is often taught with the client laying on their back, but it can be done seated, side lying, sitting, and standing as well.
Have your client lay on her back in a glute bridge position. Make sure your alignment is neutral.
As she inhales through her nose, drawing her breath up into and expanding through her rib cage.
Have her exhale like she's blowing through a straw while gently contracting her pelvic floor (only 20%-30%).
Train the deep core system and incorporate in all training and everyday life. Postpartum rehab focuses on restoring balance within that deep core system.
Refer to a Pelvic Floor Physical Therapist
A pelvic floor physical therapist is the best trained health professional to assess pelvic floor function internally both during and after pregnancy. This will give you guidance on how much impact is appropriate for your client as well as set her up for recovery postpartum.
How you train your client during pregnancy matters for her fitness return postpartum. Your client can successfully return to high impact training postpartum if you guide her to take the steps to prepare for the demands of pregnancy and birth, rehab following birth, then retrain and progressively overload when the timing is right.
Are you ready to put your personal training career into high gear? Check out ISSA's Personal Trainer Certification to become an expert in helping your clients reach their fitness goals.
Click HERE to download this handout and share with your clients!
References
National Center for Biotechnology Information (2015, Sept. 30) Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/?term=hip+flexors+stability+and+pregnancy
Hodges, Paul W.; Moseley, G. Lorimer; Gabrielsson, Anna; Gandevia, Simon C. (2003, June 3). Experimental muscle pain changes feedforward postural responses of the trunk muscles. Retrieved from https://www.bodyinmind.org/wp-content/uploads/Hodges-et-al-2003-Exp-Brain-Res-experimental-lbp.pdf